- RESEARCH
- June 2023
- Bulletin
Correction of Mandibular Prognathism
OMFS Study Compares Two Surgeries’ effects on Patients’ Quality of Life

Oral and Maxillofacial Surgery research team: Dr Mike Leung (left) and Ms Natalie Wong compare the changes of patients’ quality of life (QoL) after receiving IVRO or SSRO as the treatment for mandibular prognathism.
With a normal bite, the upper jaw and teeth sit slightly in front of the lower jaw. However, when people are described as having a long face or a prominent jaw, they may have a condition called mandibular prognathism which refers to the overdevelopment of the lower jaw. The condition is a facial deformity and affects the chewing function, facial aesthetic, and self-esteem of the individual, as well as causing jaw joint pain.
Mandibular prognathism is a rather common facial deformity in Hong Kong and Southern China, but it is relatively less frequently seen in Western countries. Orthognathic surgery is the standard treatment option for correcting mandibular prognathism, which involves surgically repositioning the lower jawbone(s) to correct the elongation of the jaw. The two most commonly used surgical techniques for mandibular prognathism correction are intraoral vertical ramus osteotomy (IVRO) and sagittal split ramus osteotomy (SSRO). IVRO is an older technique that requires intermaxillary fixation to achieve bone fixation, i.e. locking the upper and lower jaws with wire, for 6 weeks. Patients undergoing IVRO can only take fluid diets during this period. SSRO, in contrast, allows internal fixation using titanium plates and screws, which enables immediate jaw function after the surgery. Both techniques are commonly used in Hong Kong and Eastern Asia in treating patients with mandibular prognathism.
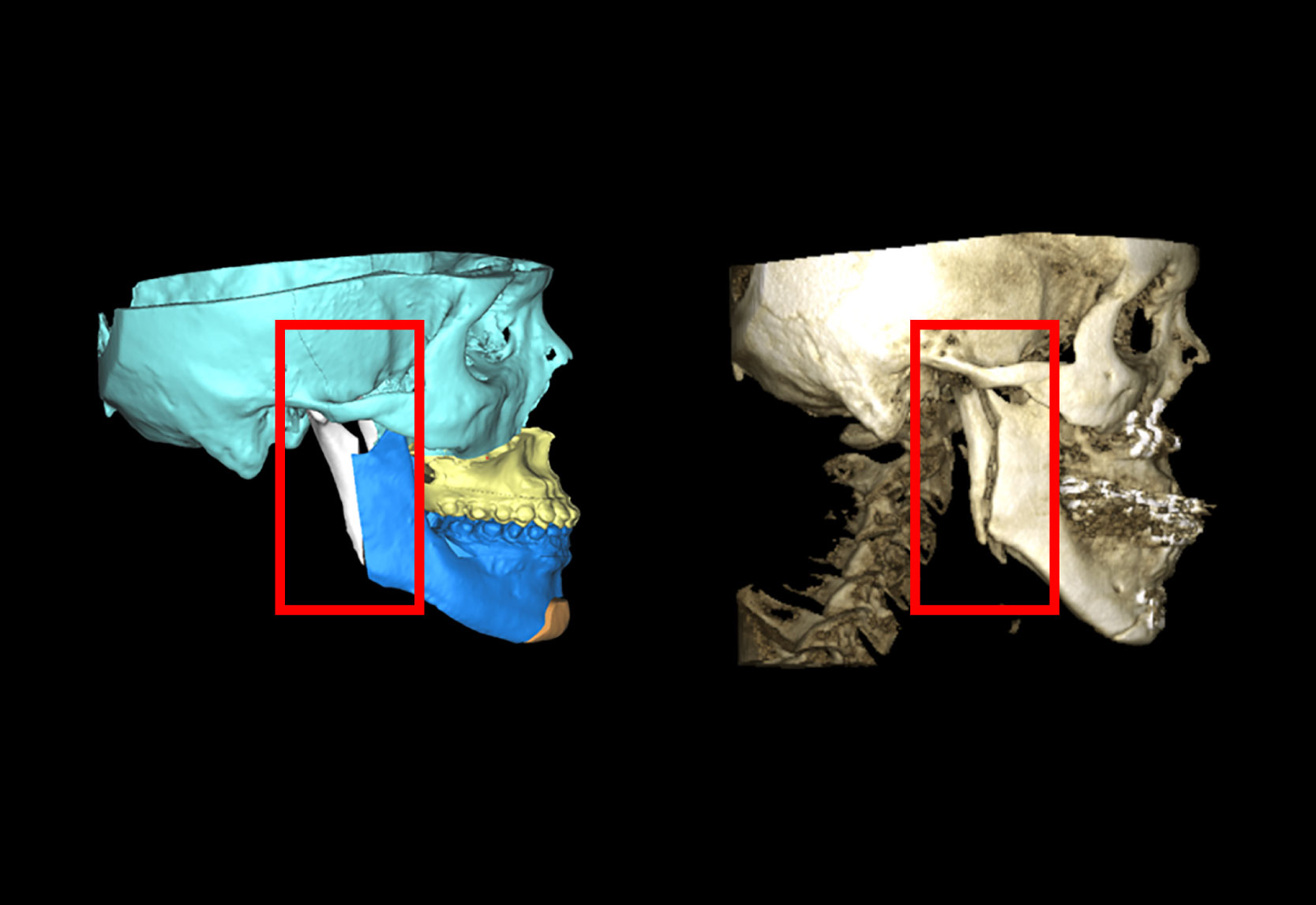
Intraoral vertical ramus osteotomy (IVRO): (Left) The pre-operative virtual surgical planning (red frame); (Right) The post-operative CT scan (red frame).
Previous studies have shown that IVRO carries less risk of injury to the nerve that supplies the lower lip sensation when compared to SSRO. SSRO may require a second small operation to remove the titanium plates and screws if they become exposed or infected. However, the need of intermaxillary fixation is a concern but was not evaluated from the patients’ perspective.
A study led by Dr Mike Leung, Clinical Associate Professor in Oral and Maxillofacial Surgery, Faculty of Dentistry, The University of Hong Kong, compared the changes of patients’ quality of life (QoL) after receiving IVRO or SSRO as the treatment for mandibular prognathism. A total of 98 patients were randomized to receive IVRO (49 patients) or SSRO (49 patients) as the mandibular setback procedure of their orthognathic surgery. The patients’ QoL were assessed using two self-administered questionnaires, namely 14-item Short-Form Oral Health Impact Profile (OHIP-14) to evaluate the oral-health related QoL, and 36-item Short-Form Health Survey (SF-36), to evaluate the physical and mental health-related QoL. The longitudinal changes of the patients’ QoL were analyzed and compared up to two post-operative years.
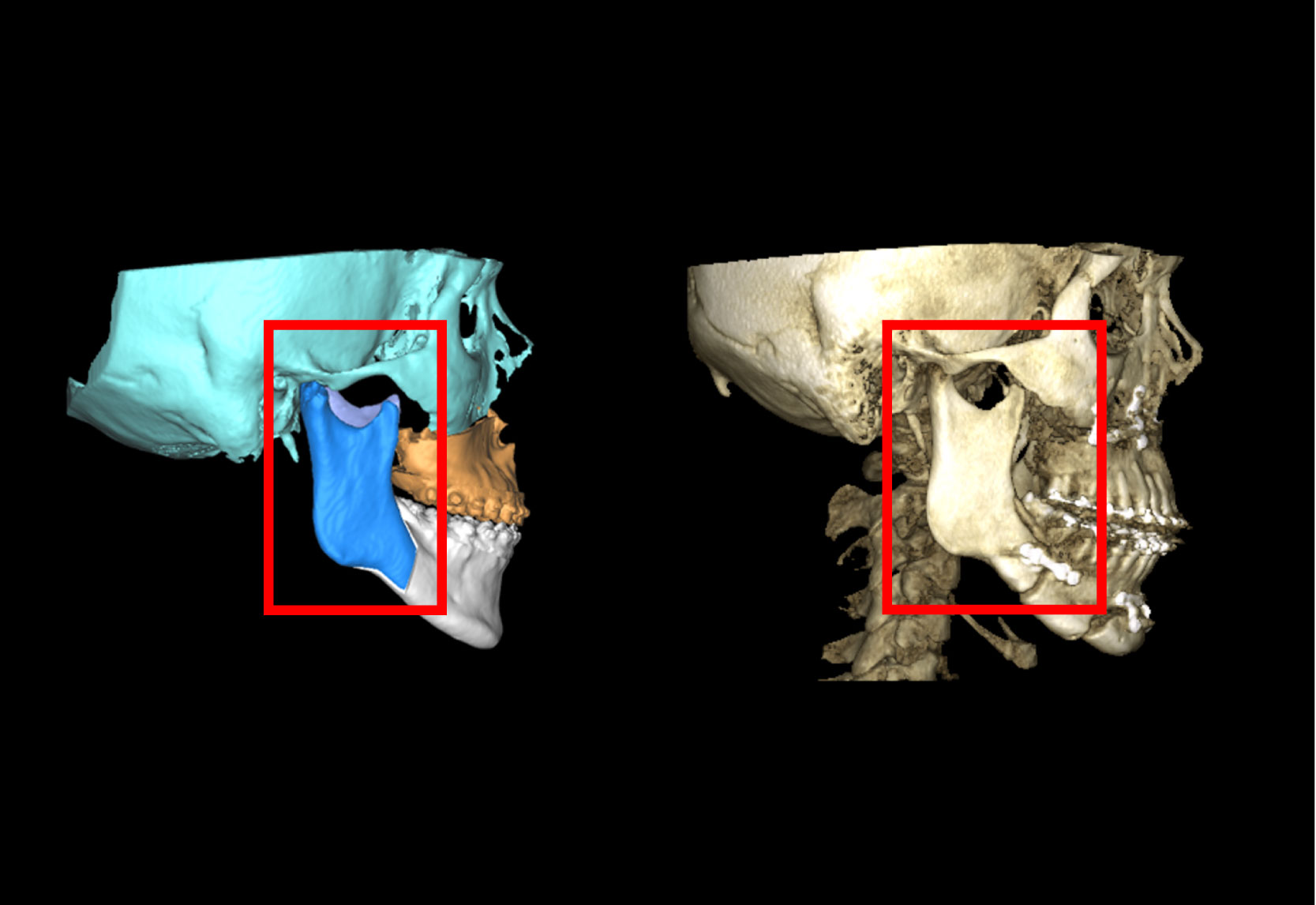
Sagittal split ramus osteotomy (SSRO): (Left) The pre-operative virtual surgical planning (red frame); (Right) The post-operative CT scan showing the fixation with titanium plate and screws (red frame).
The study found that, after an early recovery period from the surgery, the oral health-related QoL of patients of both IVRO and SSRO groups were significantly better from post-operative 3 months onwards when compared to the pre-operative status and continued to improve steadily afterwards. Besides, it was found that patients who underwent the surgery at younger ages had a better oral health-related QoL during the postoperative period.
In terms of physical and mental health-related QoL, it was found that the burden of physical impact was bigger than the psychological impact in both groups during the early postoperative period. Social functioning, emotion, and mental health specifically affected patients in the IVRO group. These findings suggested that mental health was continuously affected during the intermaxillary fixation period. Eventually, physical and mental health–related QoL of patients in both groups were able to return to baseline level or even better 2 years after the surgery. The study showed that IVRO and SSRO could both improve patients’ physical and mental health in the long term.
It is encouraging to see that the correction of mandibular prognathism improves the patients’ quality of life. The study confirms that SSRO appears to offer earlier improvement on the patients’ quality of life after orthognathic surgery because of better function.
When comparing the two surgical procedures, it was found that the patients who had SSRO had earlier improvement than those who had IVRO in the oral health-related QoL and the physical and mental health-related QoL. Patients in the SSRO group showed signs of improvement as early as 2 weeks after the surgery, which could be related to the earlier mobilization and resumption of functions like mastication and speech without the need of intermaxillary fixation.
“It is encouraging to see that the correction of mandibular prognathism improves the patients’ quality of life,” Dr Leung explained, “The study confirms that SSRO appears to offer earlier improvement on the patients’ quality of life after orthognathic surgery because of better function.”
“It is important to understand how different surgical procedures for treating mandibular prognathism affect the patients from their perspective,” Ms Natalie Wong, Co-investigator of the study, said “On top of knowing the clinical outcomes like stability and possible risks of the two procedures, this study reflected how the surgical procedures may impact their quality of life from different dimensions.”